A rich text element can be used with static or dynamic content. For static content, just drop it into any page and begin editing. For dynamic content, add a rich text field to any collection and then connect a rich text element to that field in the settings panel. Voila!
Headings, paragraphs, blockquotes, figures, images, and figure captions can all be styled after a class is added to the rich text element using the "When inside of" nested selector system.
Here is another list:


CPR in a moving vehicle means performing chest compressions and rescue breaths inside a car, van, ambulance, or other transport when someone is unresponsive and not breathing. The goal is to maintain blood flow and oxygen until professional help or advanced life support is available.
Early Cardiopulmonary Resuscitation is critical because brain damage can begin in 4–6 minutes and death can occur within minutes if care is delayed. Drivers, passengers, EMTs, and first responders must understand how vehicle movement, limited space, and safety risks affect CPR effectiveness.
This article explains the major challenges of performing CPR inside a vehicle, including tight cabin space, ongoing motion, equipment access, rescuer safety, and legal considerations. It also provides step-by-step guidance for different vehicle types and answers common questions about real-world scenarios.
Proper CPR training significantly improves outcomes. Completing a recognized online CPR certification, such as ATAC’s program, gives learners structured practice, updated guidelines, and confidence to respond during emergencies.
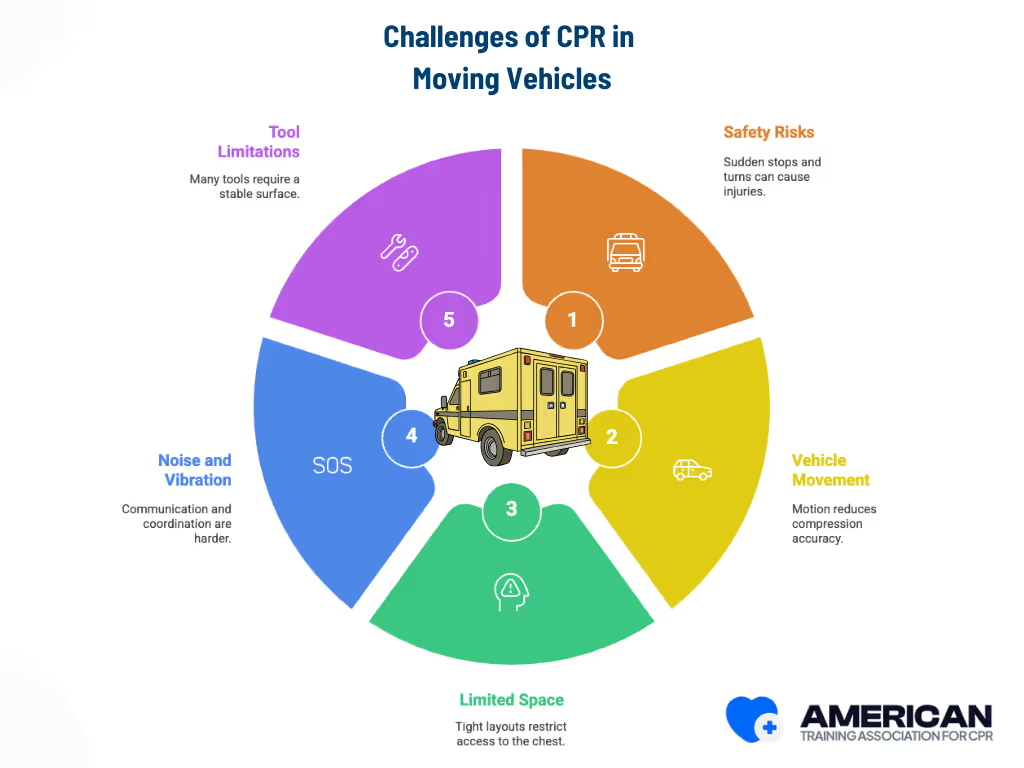
CPR in a moving vehicle is hard because safety risks, vehicle movement, and limited space make high-quality compressions difficult. According to EMS transport studies, sudden stops and turns can injure both the rescuer and the patient, and motion significantly reduces compression accuracy while increasing rescuer fatigue. Research on in-ambulance CPR performance shows that tight cabin layouts restrict access to the chest and airway, and noise and vibration make communication and coordination harder for the resuscitation team. Guidance from emergency medical services safety organizations also notes that many CPR tools require a stable surface, limiting what can be safely used during transport. These combined factors make in-transit CPR highly challenging and influence the legal and operational decisions rescuers must consider.
CPR in a moving vehicle involves significant legal and safety risks, and the safest option is to stop the vehicle whenever possible. According to EMS safety research, CPR quality declines when rescuers perform compressions in motion, and compression depth becomes inconsistent on a moving stretcher or vehicle floor. Studies have also shown that providers frequently lose balance and experience back strain during transport, which increases the chance of rescuer injury.
Legal concerns include liability, standards of care for licensed providers, and Good Samaritan protections for bystanders. These factors guide decisions toward reducing foreseeable harm and following local laws and employer policies.
Stopping is required when the patient is unsecured, compression quality drops below 100–120 per minute at 5–6 cm compression depth, or external hazards are present. When movement cannot be avoided, rescuers should secure the patient, brace themselves, and adjust technique to maintain safe, effective compressions.
Use gloves and a barrier device when available, balancing infection control with the need to start CPR quickly. Provide clear updates to EMS and document key times and actions, which supports coordination and reduces legal exposure.
Rescuer safety always comes first. CPR should be paused if continuing would expose the rescuer to traffic danger, fire, instability, or other life-threatening hazards.
CPR in a moving vehicle follows the standard CPR sequence but requires extra attention to safety, patient positioning, and rescuer stability.
Stop the vehicle immediately if conditions become unsafe. Transfer care to EMS as soon as they arrive. Safety always comes first when performing CPR in transit.

The first step in CPR is to determine whether the patient is responsive and breathing. Begin by confirming scene and vehicle safety, ensuring both the rescuer and patient are secure. Approach the patient and use a brief, noninvasive touch,such as a shoulder tap, while speaking loudly and clearly to ask if they are okay. Deliver a firm but gentle tap or flick to the shoulder, then simultaneously observe the chest for movement, listen for breath sounds, and feel for airflow at the patient’s mouth and nose.
When evaluating breathing, focus on chest rise, breath sounds, and airflow on your cheek. Distinguish normal, regular breathing from agonal or gasping breaths. Vehicle motion can create noise or visual distractions, so position your head close to the patient’s mouth and nose and limit the assessment to 10 seconds.
This step establishes the patient’s responsiveness and breathing status, which directly determines whether to proceed to calling for Help and begin emergency interventions.
Call 911 or local emergency services immediately. A designated passenger should report the emergency, the exact location (highway, exit, mile marker, intersection, or GPS), that the patient is unresponsive and not breathing, and that CPR is in progress. Place the phone on speaker so updates can continue while compressions are performed.
If two or more rescuers are present, assign one as the caller and another as the compressor. The compressor continues chest compressions or the 30:2 cycle per dispatcher instructions, rotating every two minutes or sooner if fatigued.
Tell dispatch the vehicle location, whether it is moving or stopped, direction of travel, number of patients, and any cabin limitations. Keep statements brief to avoid interrupting compressions.
Use hands-free options such as a Bluetooth headset, speakerphone, or dashboard mount. If service is poor, give nearby landmarks or mile markers. Always keep the caller at the phone and do not remove the compressor from the patient.
Positioning the patient properly ensures safety and allows effective chest compressions in a moving vehicle. Focus on selecting the most stable seat, stabilizing the head and neck if spinal injury is suspected, securing the patient to minimize motion, and placing the rescuer in a safe and effective position. Avoid unnecessary repositioning that could increase injury risk or interrupt CPR.
Avoid unnecessary repositioning that could cause further injury or interrupt CPR. Move the patient only when it is safe, with manual spinal stabilization and adequate help.
Chest compressions must remain high quality even in a moving vehicle. Focus on proper rate, depth, hand placement, and rescuer stability. Minimize interruptions, plan smooth team handovers, and stop only when vehicle motion makes compressions unsafe. Resume immediately when conditions allow.
Maintain 100–120 per minute and 5–6 cm depth as the primary performance targets throughout transport.
Rescue breaths help provide oxygen while compressions maintain circulation. In a moving vehicle, trained rescuers should give breaths only when it is safe, using barrier devices when available. Keep pauses brief and maintain a stable position to avoid losing airway control.
Pull over at the next safe location if vehicle motion makes airway control unsafe. Rotate rescuers every 2 minutes to prevent fatigue and maintain effective technique. Move smoothly toward the next step: attaching and using the AED as soon as possible.
Using an AED in a moving vehicle is critical for restoring a shockable rhythm, but cabin space and motion make pad placement and shock delivery more challenging. Focus on safety, proper pad application, and minimizing interruptions to CPR.
Proper AED use in a moving vehicle requires standard defibrillation steps plus added safety precautions. After delivering shocks and resuming CPR, the next section will explain how to adapt CPR techniques for different vehicle sizes.

CPR must be adjusted based on the vehicle environment because space, access, stability, and equipment vary. Below are practical adaptations for cars, vans, buses, and ambulances, focusing on patient positioning, compression technique, rescuer posture, and safety.

Performing CPR in a moving vehicle requires balancing rescuer stability with patient protection. The following tips provide step-by-step actions to maintain effective compressions while reducing risks from vehicle motion, cabin hazards, and equipment placement.
After the event, hand over patient details to EMS, check rescuer well-being, mark hazards, and seek emotional support if needed.

Stopping CPR in a moving vehicle should be guided by patient status, rescuer safety, and operational constraints. The highest priority is return of spontaneous circulation (ROSC), confirmed by a central pulse, spontaneous breathing, and purposeful movement, or via monitors when available. CPR can also be stopped once qualified EMS providers are ready to assume care, or if a valid advance directive or formal pronouncement of death is verified. Rescuer inability to maintain high-quality compressions or the emergence of immediate dangers such as vehicle hazards justifies cessation. In cases of uncertainty, it is safest to continue compressions until one of these clear criteria is met. Proper handover and documentation ensure safe transition of care and legal compliance.
The ATAC CPR certification prepares participants to perform effective CPR in a variety of situations, including moving-vehicle scenarios, through comprehensive online training. The program focuses on knowledge, decision-making, and procedural readiness rather than physical hands-on practice. Learners gain clear instruction on CPR fundamentals, rescue breaths, AED use, patient positioning, and safety considerations in confined or transport environments.
The online curriculum uses scenario-based guidance, instructional videos, and interactive assessments to ensure participants understand how to adapt CPR techniques for different vehicle types, prioritize rescuer and patient safety, and know when to stop or adjust care. Certification validates understanding, situational judgment, and readiness to act safely under constrained conditions.
Yes. CPR in a moving vehicle can be effective if rescuers maintain high-quality compressions (100–120 per minute, 5–6 cm depth for adults) and minimize interruptions. Vehicle speed, road conditions, and rescuer stability all impact effectiveness. Stop on a safe, flat surface outside the vehicle if quickly accessible for optimal results.
Effective team leadership is critical during sudden cardiac arrest, especially in out-of-hospital cardiac arrest situations or during ambulance transport. A team leader oversees task allocation, monitors manual chest compressions for correct compression rate and compression fraction, coordinates airway management, and communicates with emergency medical services. Rapid AED use and maintaining uninterrupted compressions support delivery of oxygen-rich blood to the brain and heart. Structured leadership and vehicle-specific CPR training enhance resuscitation quality, reduce errors, and improve survivor outcomes, including survival to discharge and neurological status
Position the patient supine on the flattest available area (flattened rear seat or floorboard) with head supported for airway openness and chest exposed for perpendicular compressions. Adjust seatbacks or consider rapid removal to an external flat surface if cabin space limits access.
In confined spaces, maintain compression quality by adjusting your posture, bracing your knees, aligning your shoulders over your hands, and using shorter, forceful compressions if full arm extension is limited. Rotate rescuers frequently to reduce fatigue and preserve effective compressions despite spatial constraints.
If the patient must be moved, use proper lifting techniques with at least two trained responders. Balance spinal protection with access for effective compressions.
Provide a concise summary including time of collapse and CPR start, number and timing of shocks, airway and medication interventions, observed vital signs, and any ROSC. Clear communication ensures safe transfer and continuity of care.
During ambulance transport, rescuers should focus on maintaining high-quality cardiopulmonary resuscitation, primarily using manual chest compressions, as the American Heart Association (AHA) 2025 update no longer recommends routine use of mechanical CPR devices. Key steps include maintaining proper hand position, aligning the shoulders over the sternum, keeping the correct compression rate (100–120 compressions per minute), and rotating rescuers to reduce fatigue.
Additional strategies include securing the patient and team with stabilization straps, bracing knees, and using feedback devices when available to monitor compression depth, rate, and compression fraction.
Following AHA guidelines ensures interventions reflect current resuscitation science, improving patient outcomes and survival to discharge, even under the challenges of vehicle motion and turbulence.


